by John Fiore, PT
Runners are well aware of the importance of strength training to reduce injury risk. Even the most specific strengthening program will fail to produce results, however, if compensatory movement patterns are not addressed. Our modern lifestyle is filled with sitting. We sit at work, sit while driving, sit for relaxation, yet expect our hips, pelvis, and spine to function normally. Hip flexor tightness is synonymous with prolonged sitting. The psoas is in important hip flexor muscle which warrants further discussion to understand the challenge of running injury treatment and prevention.
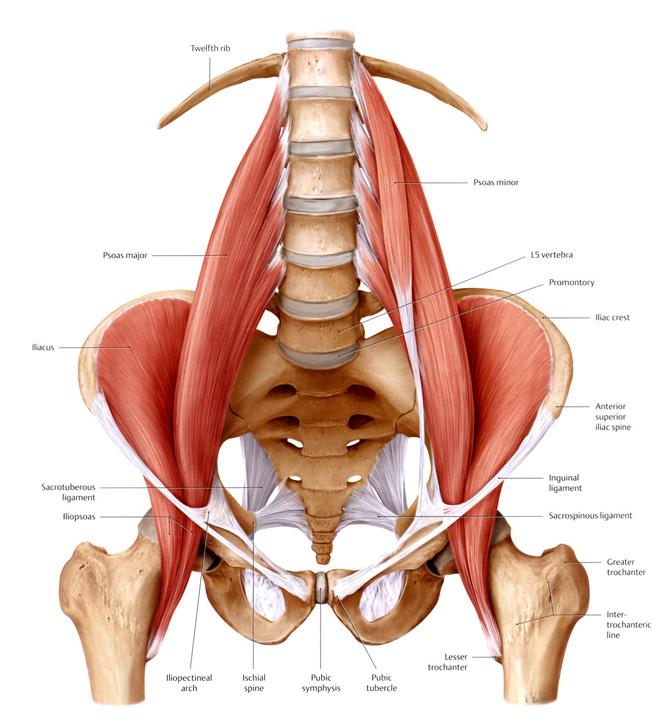
The psoas is an important core muscle which stabilizes and moves both the lumbar spine and the lower extremity. Collectively, the psoas and iliacus muscles are referred to as the iliopsoas muscle group. The psoas works in conjunction with the iliacus muscle. While both the psoas and iliacus insert on the lesser trochanter of the femur (groin area), the iliacus originates in the iliac fossa and iliac crest of the pelvis and sacrum, whereas the psoas originates along the transverse processes of the lumbar spine. The primary function of the psoas muscle is to flex the hip. Secondary actions which are very important for proper lumbar spine and lower extremity function and symmetry include femoral lateral rotation, lumbar extension, and lumbar side bending. In addition, the iliacus tilts the pelvis anteriorly. Both the psoas and iliacus muscles activate unilaterally or bilaterally. Asymmetry between the right and left psoas muscles due to tightness or weakness, therefore, is an important source of one-sided low back and leg pain. While psoas asymmetry is often overlooked, proper, targeted clinical testing must be included when thoroughly evaluating low back and extremity pain and overuse injuries.
The psoas muscle lifts the hip and leg forward when we walk, run, and climb. Overutilization of the iliopsoas can lead to postural and mechanical issues. Without the necessary strength in the abdominals, hips, gluteal and small stabilizing lumbar (multifidi) musculature, the psoas becomes shortened, over-active, and irritated. Gait and postural deviations may present as a laterally-rotated hip, an anteriorly tilted pelvis (unilaterally or bilaterally), or a sway back posture. An iliopsoas-dominant athlete may develop a myriad of overuse injuries including: psoas or groin pain, sacroiliac and low back pain, iliotibial band pain, and even knee and foot overuse injuries.
Once a psoas imbalance or overutilization issue is diagnosed, the resulting mechanical asymmetry must be addressed through manual physical therapy techniques. Targeted active release stretching, dry needling, deep tissue release, and muscle energy techniques are effective ways to restore symmetry and proper function to the right and left psoas musculature. Manual therapy alone, however will not “fix” the problem. Strengthening the antagonist musculature will allow the body to maximize efficiency of movement.
 Strengthening the weak links in the modern day athlete can be difficult due to ingrained movement patterns. Strengthening the lower abdominal and gluteal musculature, for example, reduces our reliance on the psoas to “pick up the slack” in lumbar and pelvic stabilization. Functional core strengthening involves the gluteal and abdominal musculature stabilizing in conjunction with sport-specific upper and lower extremity motions. Sit-ups and crunches alone, however, may exacerbate the problem of tight or dominant psoas musculature. It is important, therefore, to include planks (prone and side positions) and single leg weight bearing core exercises to reduce habitual psoas use. Finding your lower abdominals (transversus abdominis) muscles when lifting is key to prevent the anterior pelvic tilt associated with iliacus activation as well as the lumbar sway back associate with psoas activation.
Strengthening the weak links in the modern day athlete can be difficult due to ingrained movement patterns. Strengthening the lower abdominal and gluteal musculature, for example, reduces our reliance on the psoas to “pick up the slack” in lumbar and pelvic stabilization. Functional core strengthening involves the gluteal and abdominal musculature stabilizing in conjunction with sport-specific upper and lower extremity motions. Sit-ups and crunches alone, however, may exacerbate the problem of tight or dominant psoas musculature. It is important, therefore, to include planks (prone and side positions) and single leg weight bearing core exercises to reduce habitual psoas use. Finding your lower abdominals (transversus abdominis) muscles when lifting is key to prevent the anterior pelvic tilt associated with iliacus activation as well as the lumbar sway back associate with psoas activation.
Our modern day lifestyle of prolonged sitting and very little physical activity other than our “workouts” predisposes us to psoas muscle shortening and dominance. Sitting inherently shortens the psoas while the antagonist muscle (gluteus maximus) is unable to function the lengthened position of sitting. The most common area of weakness in present day athletes (based upon my empirical evidence of 24 years in practice) are the gluteus medius and gluteus maximus. No wonder we have difficulty contracting our gluts when much of our day is spent sitting! In addition to a physical therapy strength and postural evaluation, a video gait or running analysis will reveal muscle imbalances to address to effectively prevent and treat injuries related to a hip flexor or psoas domain state.
Finally, for an aging athlete or individual, hip joint compression due to excessive sitting and associated psoas tightness can accelerate osteoarthritis. Balancing proper muscle flexibility with core stabilization and strength will decrease the impacts of prolonged sitting to permit a healthy, active lifestyle for years to come.
(John Fiore is the owner of Sapphire Physical Therapy in Missoula. You can reach him at john@sapphirept.com or 406-549-5283)
ARTICLE REFERENCES
- McGill,S.(2007) Low Back Disorders: evidence-based prevention and rehabilitation. 2nd ed. Human Kinetics. Champaign, IL. P 60-61, 214-217.
- Jones,S. Rivett,D. (2004) Clinical Reasoning for Manual Therapists. Elseier Butterworth Hinemann. New York, NY. P 261-274,
3. Greives. Grieve’s Modern Manual Therapy. Harcourt Publishers Ltd. 19943 - http://www.serola.net/research-entry/iliopsoas/











